V
主页
20220322 IPMN(胰腺导管内乳头状黏液肿瘤)
发布人
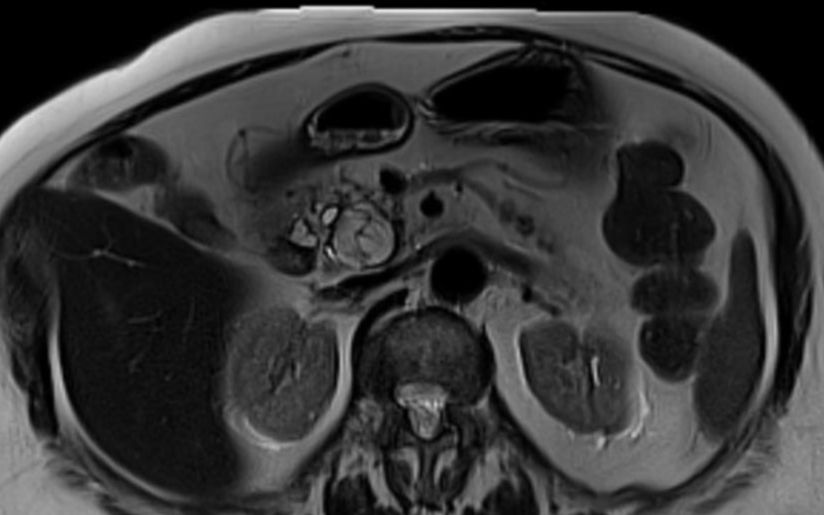
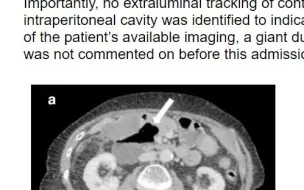
IPMN Pathophysiology An IPMN represents a potentially malignant neoplasm arising from mucin-producing cells within the pancreatic ducts. As such, the excessive amounts of mucin produced enter and dilate the pancreatic ducts. IPMNs can arise from the side branches or the main pancreatic duct, with main duct being more high risk. Lesions may be low grade or indolent lesions, with possible progression to borderline, high-grade dysplasia and invasive carcinoma. Epidemiology IPMNs typically affect an older population, with individuals diagnosed between the ages of 50 to 70 years old. They have a slight female predominance, with studies reporting ratios from 2-to-1 to 3-to-1. Other associations include cigarette smoking, diabetes, family history of pancreatic cancers and genetic syndromes, which increase the risk of gastrointestinal malignancy, such as familial adenomatous polyposis syndrome. Clinical presentation Most patients have no symptoms at the time of diagnosis, with lesions detected on imaging for other reasons. Imaging features IPMNs on CT appear as cystic lesions, typically identified when they measure under 1 cm. They may have thin septations, but low-grade lesions should not have soft tissue components. They rarely calcify. Given their small size at detection, IPMNs are best evaluated on MR. They present as cystic lesions (high T2 signal) with no enhancement; any septations also should not demonstrate thickness, nodularity, or enhancement. Dilation of the main pancreatic duct, enhancement, and interval growth are high-risk stigmata that suggest malignant transformation. Treatment Most patients are treated conservatively, given the slow progression and low risk of malignant transformation. Follow-up can vary, as there is no clear guideline. Some (such as the Fukuoka guidelines) recommend cross imaging, preferably MR, every one to two years for 10 years to establish a benign pathophysiology. For those with enlarging lesions, main duct dilation, or new
打开封面
下载高清视频
观看高清视频
视频下载器
杨敏洁:通过征象读懂肌骨影像(2) ——骨关节损伤影像学征象
《影像秒杀病例图谱(第四版)》病例2.11-2.20(肌骨影像学)
Essentials of Breast Imaging T1-CBR06
RSNA 2022:泌尿生殖系统病例多学科讨论(Genitourinary Case-based Multidisciplinary Review)
(专家读片会4、核医学+肌骨系统)Image Interpretation Session4- Nuclear Medicine and MSK
20220503_女,66岁,发现脾脏病变
20220618_男,62岁,进行性认知下降
胰腺的规范扫查技巧
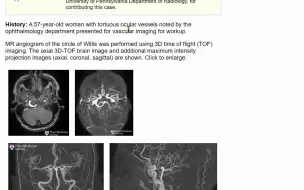
20220603_57岁,女,偶然发现眼底血管异常
ASHNR Webinar #5甲状腺影像学
(快速射击:60分钟读完80个心脏影像学病例)Rapid Fire- 80 Cardiac Cases in 60 Minutes
RSNA2022:BI-RADS下一版更新-钼靶、超声与磁共振(BI-RADS Next Edition Update)
20220508_女,10岁,半昏迷
(乳腺影像病例复习2)Case-based Review of the Breast2 - RSNA
Management of Cystic Pancreatic Lesions
RSNA2022:胸部影像学指南与科研的实用更新(Practice Updates in Chest Imaging Guidelines and Resear
Mentored Cardiac Case Review Imaging the Heart Imaging Techniques, Anatomy and F
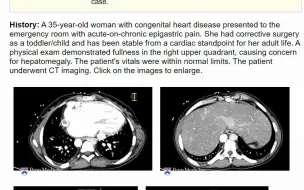
20220505_女,35岁,有先心病史,慢性上腹痛急性发作
Prostate MRI and Molecular Imaging Core and Advanced Applications
20220618_女,82岁,上腹痛.mp4
Demystifying Postoperative Spine Imaging Imaging Techniques and Case Based Revie
Aortic Dissection - S1-CVA08
RSNA2022:痴呆的病因诊断(RSNA/ESR Symposium Imaging of Neurodegenerative Disorders)
33 Pediatric Neuroradiology
男,10岁,外伤。第二掌骨基底部副骨化中心(0001284696
《影像秒杀病例图谱(第四版)》病例1.11-1.20(儿科影像学)Aunt Minnie's Atlas and Imaging-Specific Diagno
President's Address and Opening Session - S6-PL01 -
20220318急性头痛的影像学(下)
第二届飞图杯全国网络读片大赛总决赛(广州,2023/3/26 8:30AM)
Crohn's Disease Imaging M1-CGI02
(胎儿影像学)Fetal Imaging _ RSNA 2021
51 - Infections_标清
RSNA2022:儿科消化及泌尿生殖系统影像学(Pediatric GI/GU)
GI Post-Operative Imaging T8-CGI09
Non-traumatic Thoracic Emergencies
RSNA2022:急性与慢性肺损伤的影像学(Acute and Chronic Lung Injury)
RSNA2022:儿科MDT病例复习(Pediatric Case-based Multidisciplinary Review)
20201205Miss2(重要诊断,切勿漏诊!——泌尿生殖系统、头颈部及肌骨系统)
24 (超声病例复习)Unknown Case Review
The Leiomyosarcoma vs Leiomyoma The Case for Multiparametric MRI